[HIDE]
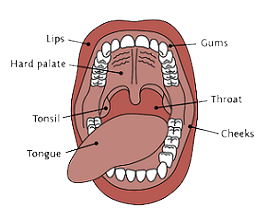
Carcinoma of the oral
cavity includes carcinoma of the tongue (about 35 per cent), carcinoma of the
floor of mouth (about 25 per cent), carcinoma of the buccal mucosa (about 15
per cent), carcinoma of the lower alveolus (about 15 per cent), carcinoma of the
upper alveolus (about 5 per cent) and carcinoma of the hard palate (about 5 per
cent). Men are more affected by carcinoma of the oral cavity than women. Risk
factors of the oral cavity carcinoma include tobacco smoking and tobacco &
betel nut chewing. Studies have shown that smokers have 10 times higher risk of
the oral cavity carcinoma. Chronic and excessive consumption of alcohol is
another risk factor. The ill-fitted denture may lead to the oral cavity
carcinoma due to chronic abrasion of the buccal mucosa. It is also associated
with poor dental hygiene and certain nutritional factors such as deficiency of
vitamin A and vitamin B. The leukoplakia (whitish patch) and the erythroplakia
(red velvety patch) are pre-cancerous conditions of the oral cavity carcinoma.
Carcinoma of the oral cavity usually presents with a red patch having ill-defined margins that may be slightly raised. It may present as a lump in the mouth that is felt with tip of the tongue. In some cases, the oral cavity carcinoma presents as a non-healing ulcer.
Staging of the oral cavity carcinoma is done as follows:
Procedures used to diagnose the oral cavity carcinoma include local physical examination, X-rays, CT scan and biopsy.
Carcinoma of the cheek
is usually a squamous cell carcinoma that usually affects heavy smokers,
alcoholics and tobacco & betel nut chewers, especially those, who plug
these contents in their cheek pouch. Chronic abrasions of the buccal mucosa by
a rough tooth or an ill-fitted denture may cause carcinoma of the cheek. A
leukoplakic patch on mucosal surface of the cheek is a major risk factor of
carcinoma of the cheek. It usually metastasises to the submandibular, submental
and the upper deep cervical lymph nodes. The diagnosis is confirmed by biopsy.
Carcinoma of the lip
usually affects elderly persons. Its incidence is ten times higher in men
as compared to women. Carcinoma of the lower lip is more common. Smoking and
ultraviolet radiation are two major risk factors. A hyperkeratotic patch formed
on the lip in smokers usually transforms to carcinoma of the lip. Ultraviolet
radiation leads to the formation of whitish tinge on the lip that is followed by
repeated cracks and desquamation causing erosions. This lesion, known as
actinic cheilitis, may transform into carcinoma of the lip. Carcinoma of the
lip usually presents with a lesion having ulcerating centre and everted
margins. Carcinoma of the lip usually metastasises to the submental and the
submandibular lymph nodes. The diagnosis of carcinoma of the lip is usually
confirmed by biopsy.
Carcinoma of the tongue is usually a squamous cell carcinoma. Risk factors of the tongue carcinoma include smoking, alcoholism, poor oral hygiene, chronic superficial glossitis, sessile papilloma and Plumer Vinson syndrome. The tongue carcinoma usually presents as an oval, raised and papillated plaque on the tongue along with excessive salivation. The lesion is usually ulcerating having indurated base and raised everted margins. Sometimes, the tongue carcinoma presents as a fungating growth. Carcinoma of the tongue remains asymptomatic in the early stages. In later stages, there may be pain and difficulty in swallowing. In the advanced stage, the tongue becomes stiff and partially fixed. There may be offensive foul smell, starvation, cachexia and bronchopneumonia. The enlarged lymph nodes and oedema of the glottis may exert pressure on the trachea leading to asphyxia. Haemorrhage may occur from the tumour or the eroded carotid artery. Carcinoma of an anterior two-third portion of the tongue may invade the mandible and floor of the mouth across the midline. Involvement of muscles of the tongue may affect the speech. Ultimately, the tongue may become fixed due to extensive infiltration of the tumour into the floor of the mouth. Carcinoma of posterior one-third of the tongue may involve the tonsils, pharynx, cervical spine, soft palate, epiglottis and the larynx. Carcinoma of the tongue usually metastasises to the submandibular lymph nodes. The diagnosis is confirmed by biopsy.

Disclaimer:
This content is for information and educational purposes only and should not be perceived as medical advice. Please consult a certified medical or healthcare professional before making any decision regarding your health using the content above.
Click here to go back to the list of all Articles


Oral Cancer (Carcinoma of the Cheek, Lips & Tongue)