[HIDE]
Common types of skin cancer include basal cell carcinoma arising from the basal cells; squamous cell carcinoma arising from the squamous cells; and malignant melanoma arising from the melanocytes. Kaposi's sarcoma and mycosis fungoides are other cancers of the skin. Exposure to ultraviolet radiation is considered as the most common cause of skin cancer. Other causative factors of skin cancer include exposure to radium, coal tar and arsenic compounds. The people with fair complexion and those living near equator have the highest risk of skin cancer. Incidence of skin cancer is much lower in black races due to a higher content of melanin in their skin.
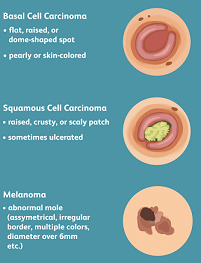
Basal cell carcinoma is the most common cancer of the skin. It is a low-grade, slow-growing cancer that usually occurs in the fair coloured people during old age. Exposure to ultraviolet radiation is considered as the major risk factor of basal cell carcinoma of the skin. In about 90 per cent cases of basal cell carcinoma of the skin, the lesion develops on the face, usually above an imaginary line drawn from lobe of the ear to corner of the mouth, particularly around inner canthus of the eye. Basal cell carcinoma of the skin usually presents as a nodular, non-ulcerating, dark translucent lesion. Some lesions are ulcerating with raised rolled margins, which heal temporarily and again start ulcerating along with a serous discharge or bleeding. The lesions gradually erode the deeper tissues such as the muscle, cartilage and the bone. Sometimes, basal cell carcinoma of the skin presents as a red shiny plaque on the back of the trunk. Basal cell carcinoma of the skin may transform into the squamous cell carcinoma. Diagnosis of basal cell carcinoma of the skin is confirmed by biopsy.
Squamous cell carcinoma of the skin is comparatively less common but more malignant than the basal cell carcinoma. It usually occurs in exposed parts of the body. The incidence is higher in the fair coloured people. Squamous cell carcinoma may develop in a pre-existing skin lesion such as leukoplakia, solar keratosis and Bowen's disease. Risk factors of squamous cell carcinoma of the skin include chronic venous ulcers, chronic lupus vulgaris and prolonged irritation of the skin by chemicals. Squamous cell carcinoma of the skin usually presents as a warty, scaly lesion, preceded by keratin production. The ulcerating lesion may be irregular in outline with raised and everted margins and indurated base that is attached to the deeper tissues. There may be bloodstained discharge from the ulcer due to secondary infections. Squamous cell carcinoma of the skin usually spreads to the regional lymph nodes. Diagnosis of squamous cell carcinoma of the skin is confirmed by biopsy.
Malignant melanoma usually affects the white-skinned people and occurs at a younger age. Exposure to ultraviolet radiation is considered as the major risk factor of the malignant melanoma. Multiple episodes of sunburn in children may lead to the genesis of the malignant melanoma. Malignant melanoma usually affects the legs in women and the trunk in men. Other sites of malignant melanoma include eyes, meninges and mucocutaneous junctions. The lesions of malignant melanoma are usually flat or raised with typical irregular margins. There are many types of malignant melanoma, out of which the superficially spreading malignant melanoma is the most common. Primary malignant melanoma (lentigo malignant melanoma) usually presents as flat brown spots on the back of the hands in elderly people. Acral-lentiginous melanoma arises from the palms, soles and nail beds. Malignant melanoma should be suspected if there is itching, bleeding or change in the colour of a pre-existing mole; or there is the sudden appearance of a mole or a freckle. Extensive visceral involvement of the disease may lead to melanuria. Malignant melanoma usually spreads to the regional lymph nodes. It also metastasises to the liver, lungs, bones and the brain through the blood stream.
Staging of the malignant melanoma is done as follows:
Staging of the malignant melanoma is also done by Clark’s level:
Another method used in staging of the malignant melanoma is known as microstaging, which depicts thickness of the tumour and depth of its invasion into the skin. Diagnosis of the malignant melanoma is confirmed by biopsy.

Disclaimer:
This content is for information and educational purposes only and should not be perceived as medical advice. Please consult a certified medical or healthcare professional before making any decision regarding your health using the content above.
Click here to go back to the list of all Articles


Skin Cancer